

Please view the November 2021 Case of the Month below:
Clinical Cases from Emory Division of Hospital Medicine Annual Clinical Vignette Conference
“A Case of Secondary Priapism in Hematologic Malignancy”
Submitted by:
Hemang Shah, DO
Assistant Professor
Division of Hospital Medicine
Emory Department of Medicine
Edited by Yelena Burklin, MD, FHM, FACP
Case
A 48-year-old male with a history of DM, primary HTN, and weight loss, who discontinued all home medications in the last four months, presented with a concern for penile infection. Patient was evaluated by a primary care physician, who informed the patient of a previously diagnosed elevated blood cell count, which had progressed over the last six months. Patient reported an unintentional 60 lb weight loss over the last three months despite placing himself on a high-protein diet. A month ago, he developed priapism while on a business trip, and underwent penile decompression with the resolution of symptoms at that time.
Upon presentation, patient reported worsening pain in the penile area and recurrent priapism. Patient reported no pertinent family or social history.
He was a truck driver and was up to date with his immunizations.
Upon review of symptoms, patient reported constant severe pain in the perineal area from the base of penis to the perianal area.
Upon admission, patient was afebrile, had tachycardia up to 116 BPM and was normotensive.
His initial physical examination demonstrated frank purulent discharge from the follicles in the area of the penile shaft with concomitant skin breakdown.
Initial laboratory results revealed white blood cell count of 235.1 x 103/ µL, hemoglobin of 9.4 g/dL, and platelet count of 583,000/µL.
The images and the reported results of the abdominal, and pelvic computed tomography (CT) are provided below:
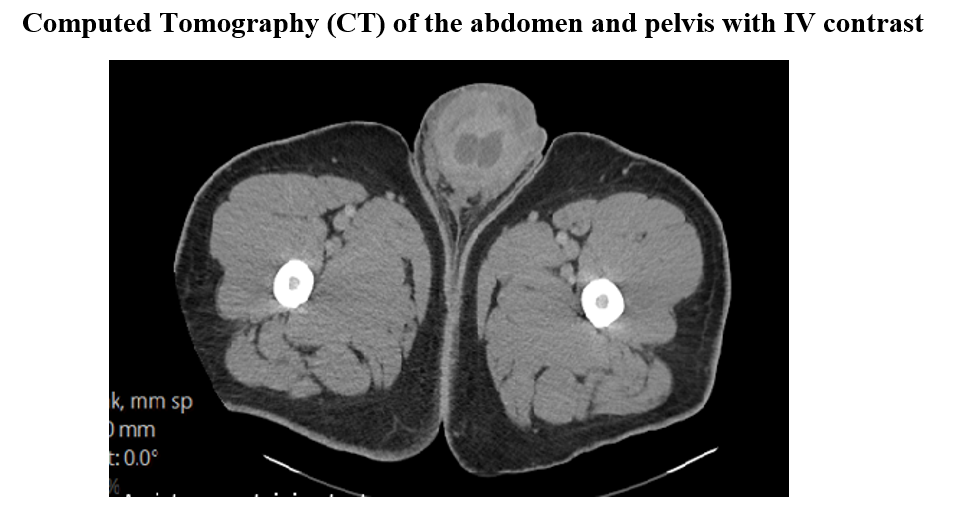
CT of the abdomen and pelvis with IV contrast revealed splenomegaly and inguinal/pelvic lymphadenopathy concerning for a lymphoproliferative disorder such as leukemia. Extensive stranding and edema of the partially imaged penile shaft was compatible with known cellulitis. There was no organizing fluid collection to suggest an abscess.
Review of 200 cells counted on a blood smear revealed marked granulocytosis, normocytic anemia, and thrombocytosis with 7% blasts and 3% basophils.
What is the diagnosis?
Chronic myeloid leukemia (CML) with a Philadelphia chromosome (Ph) generated by a translocation between the long arms of chromosomes 9 and 22 and loss of a Y chromosome.
Explanation
The morphologic and flow cytometry analysis on blood sample is compatible with chronic myeloproliferative neoplasm/rule out chronic myeloid leukemia BCR-ABL1-positive as clinically and genetically correlated.
Chromosome analysis demonstrates twenty abnormal metaphases with a Philadelphia chromosome (Ph) generated by a translocation between the long arms of chromosomes 9 and 22 and loss of a Y chromosome as seen in association with chronic myeloid leukemia.
FISH oncology cytogenetics is positive for structural abnormality, t(9;22), in 98 % of cells.
Disease Trajectory of Interest
Patient with a newly diagnosed CML was treated with a tapering dose of hydroxyurea. WBC continued to decrease, reaching 66.6 x 103/ µL upon discharge. Dasatinib was ordered for outpatient management. Rasburicase was not administered as uric acid did not increase significantly and no signs of tumor lysis syndrome were noted.
With regards to priapism, patient clinically developed woody fibrosis of the corporal bodies as well as superimposed cellulitis in the area of his prior induration at the mid-shaft. He completed antibiotic therapy, and his priapism resolved. However, given the duration and etiology of his ischemic priapism, he is likely to develop permanent erectile dysfunction.
Discussion
Priapism as a result of hematologic malignancy is most likely caused by venous obstruction from microemboli or thrombi, as well as hyperviscosity caused by the increased number of circulating leukocytes in mature and immature forms. In adult leukemic patients, the incidence of priapism is estimated to be approximately 5%. In patients with leukemia, 50% of cases of priapism are due to CML. Priapism is an andrological emergency with a poor prognosis, as the risk of impotence can be up to 50% despite appropriate management. Other hematologic diseases associated with priapism include sickle cell anemia, chronic lymphocytic leukemia, and acute lymphoblastic leukemia.
There is a paucity of data available on the correct management of priapism, and no standard treatment has been recommended for leukemic priapism. According to the American Urologic Association, systemic treatment of an underlying hematologic disorder should be undertaken in conjunction with the intracavernous management of priapism. Leukopheresis and tyrosine kinase inhibitors (TKIs) could be administered in cases of confirmed leukemic priapism.
Citations
Be the first to comment on "Faculty Development Case of the Month: November 2021"