
The Department of Medicine’s Clinical Excellence Community has introduced a new section to the monthly Clinical Excellence Newsletter. Read the new case each month and submit your response via the link below. Those with the correct answer will be listed in next month’s edition! Have a suggestion for a future case to feature? Please contact Hannah Joy at hannah.joy@emory.edu.
CLINICAL CASE OF THE MONTH:
A 54-year-old man is referred to you by his local cardiologist for further evaluation of unexplained progressive dyspnea and edema for the last few years.
He was born with cyanotic heart disease and was told that he had tetralogy of Fallot. When he was 8 years old, he had open heart surgery to repair tetralogy of Fallot that included relief of pulmonary stenosis and ventricular septal defect patch closure. His cyanosis resolved after this surgery and he did well with a relatively normal childhood and early adulthood.
Over the last 10 years, he noticed progressive lower extremity swelling. Over the last two to three years, he noticed progressive dyspnea on exertion and generalized fatigue. He now has advanced symptoms with minimal exertion.
During this time, he has been followed by his local cardiologist. Evaluation over the years included several transthoracic echocardiograms, a transesophageal echocardiogram, and a recent cardiac MRI. These have consistently showed normal left ventricular systolic function without significant aortic or mitral valve disease. The right ventricle has dilated progressively with worsening function. No obvious residual pulmonary stenosis or branch pulmonary artery stenosis was found. Nuclear stress testing was negative for obstructive coronary disease and ventilation/perfusion scan was negative for pulmonary embolus.
His medications include furosemide, spironolactone, carvedilol, lisinopril, atorvastatin, and aspirin.
Physical examination shows vital signs within normal limits. He is overweight and comfortable at rest. His neck veins are distended with increased elevation during inspiration. He has 3+ pitting ankle edema. His apex is not displaced and feels normal. His first heart sound is normal and his second heart sound is single. There is 2/6 systolic murmur and a 2/4 rapid decrescendo diastolic murmur both best heard at the base. His exam is otherwise unremarkable.
Laboratory evaluation included CBC and comprehensive chemistry that were within normal limits.
His ECG is shown here:
{kind=link}
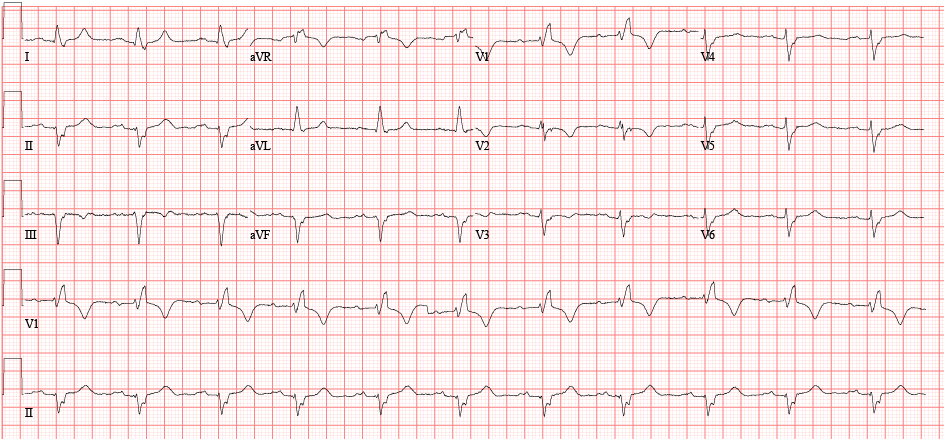

Thanks to Dr. Maan Jokhadar (associate professor of medicine, Emory University Division of Cardiology) for the Case of the Month. Brought to you by the Emory University Department of Medicine’s Clinical Excellence Community. If you are interested in investing in research, clinical care, and/or education within the Emory University Department of Medicine, please visit our website to learn how you can help.
Related Links
Be the first to comment on "Do you have the answer? Check out the new “Clinical Case of the Month”"